Over the next 18 months, Washington will scale back Medicaid (and to an extent Medicare) through tougher eligibility parameters, new work requirements for enrollment, tighter state financing options, and expanded cost-sharing for enrollees. So how will this impact Coastal Virginia?
The geographic distribution of Medicaid dependency points to structural inequalities that make the looming cuts particularly devastating. Roughly 13% of the region’s residents rely on Medicaid for health coverage.
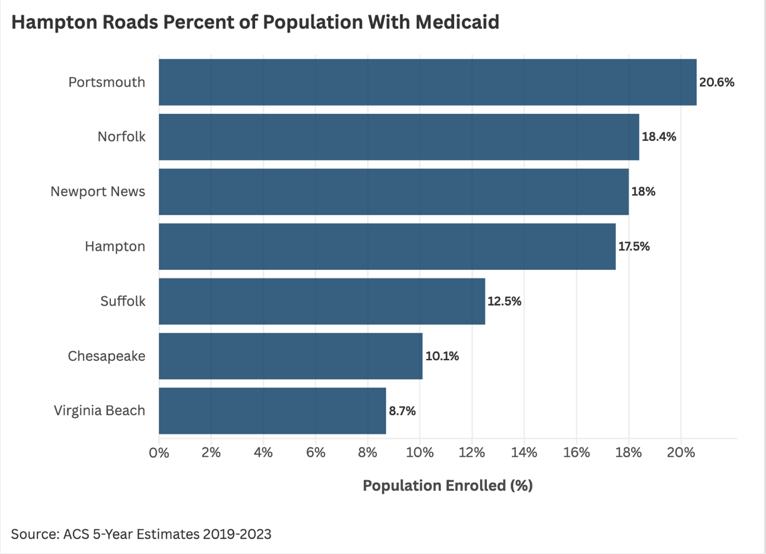
Portsmouth leads, where 20.6% of the city’s residents rely on Medicaid. Norfolk and Newport News follow, with 18.4% and 18% respectively. In Hampton, 17.5% of residents are enrolled in Medicaid. Together these four cities account for close to 111,500 of the region’s enrollees. More affluent, Whiter, cities like Suffolk, Chesapeake, and Virginia Beach tend to have less Medicaid enrollment.
Medicaid expansion in Virginia drove a sizeable increase in enrollment across Hampton Roads.
Between the 2010-2014 and 2019-2023 periods, the number of Medicaid recipients in the region grew by roughly 46%. This occurred even while the region’s total population grew by only ~3%. This nearly 16-fold difference suggests Medicaid expansion met a sizable pre-existing need for care.
At the regional level, the Medicaid coverage rate, the proportion of the entire region’s residents enrolled in the program, increased from 8.9% to 12.7%, a rise of 3.8 percentage points. That seemingly modest rate change masks the scale of the shift in absolute terms: the number of individuals dependent on Medicaid grew by nearly half in the last ten years, signaling the importance Medicaid plays in the region's healthcare landscape.
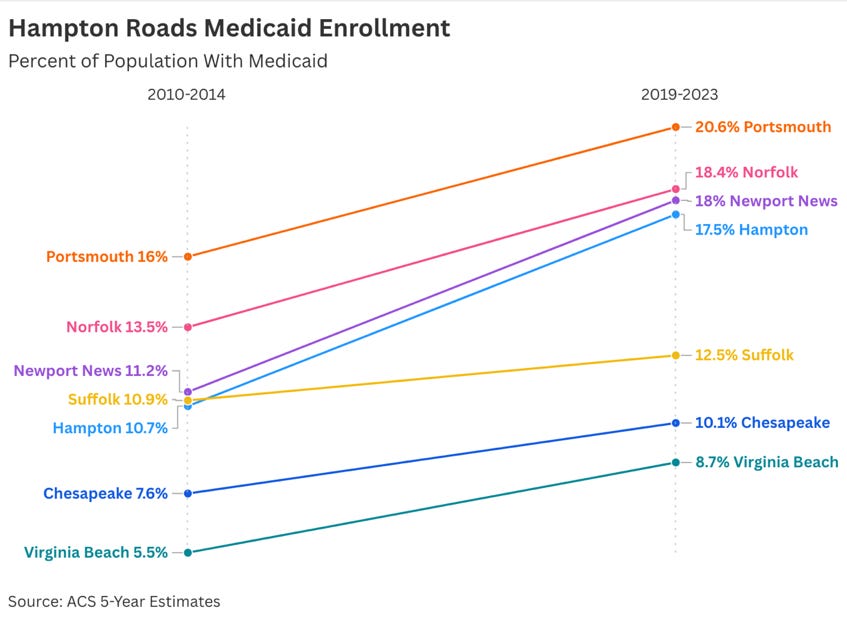
This dynamic is clearer at the city level. Hampton’s population growth was basically flat, while its Medicaid enrollment expanded by 61.5%, driving its coverage rate up 6.8 percentage points. Newport News demonstrated similar patterns, with population growth under 2% accompanied by a 63% increase in Medicaid recipients. Perhaps most notably, Norfolk lost 4% of its population while simultaneously adding over 8,000 individuals to Medicaid rolls, a 29% increase that suggests a growing erosion of economic security among residents. Even Virginia Beach, despite its relative affluence, saw Medicaid enrollment increase by 61%, adding over 14,000 residents to the program.
On the heels of Virginia’s Medicaid expansion, data suggests a sizeable drop in the region’s uninsured residents. When Virginia expanded Medicaid in 2019, the region's uninsured population fell 39.7%, from 163,794 to 98,815 people, a reduction of nearly 65,000 individuals.
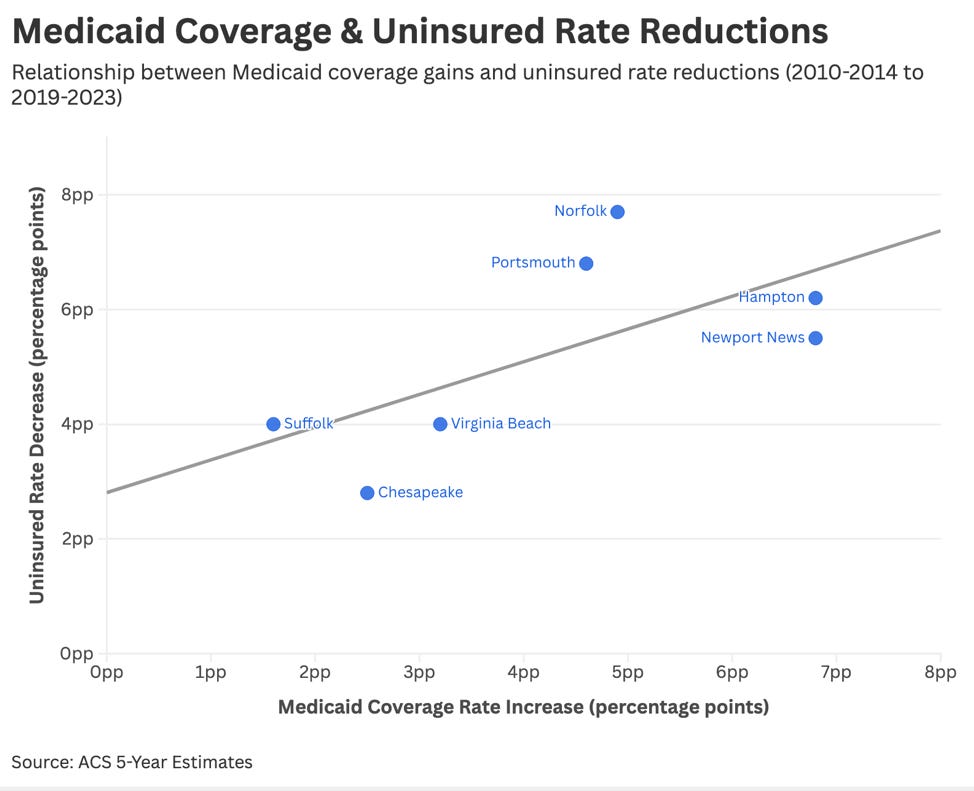
Of course, correlation is not causation. And while multiple factors contributed to this drop in uninsured rates, cities with the largest Medicaid enrollment gains did see some of the steepest reductions. In Norfolk, the uninsured rate was cut nearly in half, with the share of uninsured residents falling 7.7 percentage points from 16.8% to 9.1%, the largest reduction in the region. This translated to nearly 18,000 fewer people likely relying on emergency rooms for primary care.
Similarly, as Portsmouth’s Medicaid coverage expanded to reach more residents, the city's uninsured rate dropped by 6.8 percentage points, from 13.4% to 6.6%. In Hampton, the city’s share of total residents without insurance fell 6.2 percentage points while the share with Medicaid coverage rose 6.8 percentage points. In people terms, Hampton’s uninsured population fell from 17,000 to 9,000, basically cutting their uninsured population in half.
It’s too early to know precisely how Medicaid cuts will play out in Hampton Roads, but we’re not guessing in the dark. In 2018, Arkansas implemented a Medicaid work requirement. Within months, more than 18,000 adults, over 13% of those subject to the requirement lost coverage. This was driven largely by administrative fumbles and unclear rules rather than increased employment. A study in Health Affairs found the effort failed entirely. There was no increase in employment, and half of those who lost coverage couldn’t pay medical debts and delayed necessary care due to costs.
In Hampton Roads, similar cuts would trigger predictable consequences: thousands losing Medicaid coverage, insurance premiums rising market-wide as hospitals cost-shift uncompensated care, and an unabated public-health exigency paid for with the lives of the poor, again.